- +91 99202 00400 / +91 22 4113 6565
- contact@neurogen.in
Disclaimer: At NeuroGen BSI, autologous bone marrow tissue, after minimal manipulation, is grafted by medical practioners as part of routine procedure within the hospital in the same surgical sitting. According to the directives of the Ministry of Health and Family Welfare issued under section 33P of the Drugs and Cosmetics Act,1940 this procedure does not involve use of stem cells/ stem cell derived product.
Muscular dystrophy (MD) refers to a group of more than 30 genetic diseases which show progressive muscle degeneration causing muscle weakness. The term 'dystrophy' is derived from the Greek word "dys" which means 'difficult' or 'faulty' and "troph" which means 'to nourish'. Thus, Muscular Dystrophy implies a faulty muscle production or growth, or destruction of the muscles.
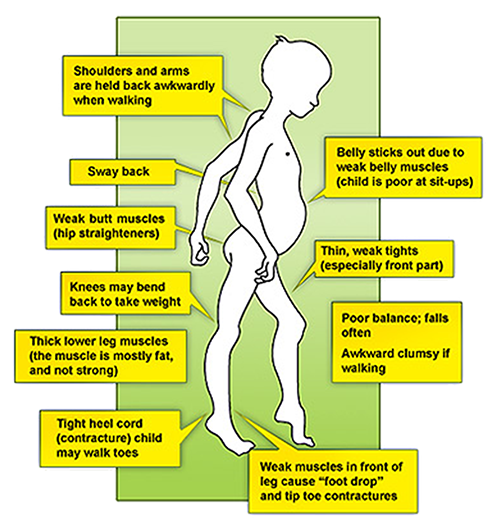
Muscle weakness is the core symptom of muscular dystrophy which leads to various postural deviations and compensations to carry out the daily functional activities. These disorders vary in age of onset, severity, and pattern of affected muscles. All forms of muscular dystrophy grow worse as muscles progressively degenerate and weaken.
All the muscular dystrophies are caused due to a core genetic defect and their. Different types are determined based on different genes and the proteins that are formed by these genes. These defects can be inherited or sporadic, which means that the disorder can be passed on from one generation to another or can occur as a spontaneous defect in the genes of an individual.
Muscular Dystrophy can be inherited in following ways: -
Autosomal dominant inheritance occurs when a child receives a normal gene from one parent and a defective gene from the other parent.

Autosomal recessive inheritance means that both parents must carry and pass on the faulty gene. The parents each have one defective gene but are not affected by the disorder.

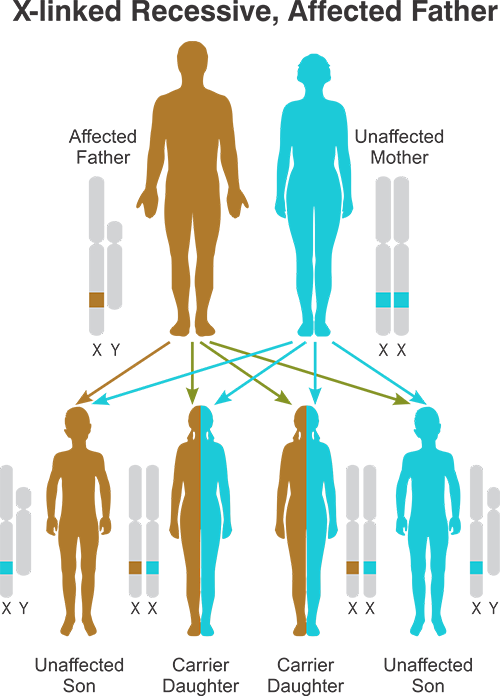
X-linked (or sex-linked) recessive inheritance occurs when a mother carries the affected gene on one of her two X chromosomes and passes it to her son.

Because of these genetic defects the proteins that are formed by these genes are either absent or less functional. The group of proteins that are affected in different muscular dystrophies are from a complex called dystrophin sarcoglycan complex (DGC). DGC is crucial to maintain the structure of the cell wall of the muscle cell, myocyte. Muscle degeneration occurs due to disruption of the cell wall of myocyte even with day to day muscle activity. This uncontrolled degeneration leads to progressive muscle death and therefore weakness, causing muscular dystrophy. Uncontrolled muscle death is the primary cause of muscle weakness however there are many other factors that hamper muscle health.

Due to continuous muscle degeneration there is chronic inflammation which damages muscles even more. As the cell that make new muscle cells are exhausted there is scarring of muscles and muscle cells are replaced with fat cells or connective tissue causing contractures. Not only in the muscles but DCG is also present in various non-muscular tissue like nerves, kidneys, spleen and schwann cells. Therefore muscular dystrophies may show some neurological symptoms as well.
Depending upon impaired gene, site where the gene is located and the progression of symptoms muscular dystrophies are divided into various types.

There are nine major forms of muscular dystrophy:
Types of Muscular Dystrophies |
Age of Onset |
Signs & Symptoms |
|---|---|---|
Duchenne (DMD) |
2 to 6 years (most severe form of Muscular Dystrophy) |
Generalised muscle weakness in all voluntary muscles ,Gower's sign positive (patient makes use of his hands to climb up on his body while getting up from floor), frequent falls while walking, poor balance in standing & walking. |
Becker's (BMD) |
Adolescence to early adulthood |
-Identical to Duchenne, but less severe; |
Limb-girdle (LGMD) |
Late childhood to middle age |
-Hip & shoulder muscle weakness
|
Facioscapulohumeral (FSHD) |
Childhood to early adulthood |
-Facial muscle weakness (eyelid drooping, inability to whistle, decreased facial expression)
|
Myotonic (DM) |
20-40 years |
-Weakness of all muscle groups accompanied by delayed relaxation of muscles after contraction
|
Congenital (CMD) |
Since birth |
-General muscle weakness
|
Oculopharyngeal (OPMD) |
40-70 years |
-Affect muscles of eyelids and throat causing weakening of throat muscles, which, in time, causes inability to swallow and emaciation from lack of food |
Distal (DD) |
40-60 years |
-Weakness and wasting of muscles of the hands, forearms, and lower legs |
Emery-Dreifuss (EDMD) |
Chilhood to early teens |
-Weakness and wasting of shoulder, upper arm, and shin muscles |
Muscular Dystrophy is a disease whose cure is still unknown to mankind even though the pathology of the disease is well understood. Conventional therapy includes drug therapy and rehabilitation.
Drug Therapy : This include those drugs which slow down the progression of muscle wasting. Anabolic steroids and supplementation are commonly used. These drugs have proven to efficacious so as to preserve pulmonary function, delaying the loss of ambulation and stabilizing muscle strength. Corticosteroids may enhance myoblast proliferation and promote muscle regeneration. Alternatively, steroids may inhibit muscle degradation by stabilizing lysosomal-bound proteases or muscle cell membranes. Finally, prednisone could reduce muscle damage and necrosis through its immunosuppressive and anti-inflammatory effects.
None of the existing medicines have shown in effect on the actual pathophysiology of the disease and provide only a moderate benefit for delaying progression of the disease.
Rehabilitation : Physical therapy, aquatic therapy, occupational therapy, speech therapy and other recreational therapies play a very important role in helping the patient to go about his daily activities and increasing their own independency. The main aim of these therapies is to maintain the muscle extensibility and prevent joint contractures that lead to deformities, thus aiming to improve quality of life of the patient.

Gene Therapy : The aim of the Gene Therapy is precisely to introduce these genes into the patients to normalize the gene expression and protein production. Although it might seem like an easy task, in reality it is quite daunting due to the complexity of human genes and gene expression. Several novel strategies for replacing or repairing the defective gene are in development, with early encouraging results from animal models. In most of the gene therapies a normal gene is inserted into the genome to replace the abnormal gene causing the disease. This can be done using viral vectors, Antisense-Induced Exon Skipping or Read through Stop Codon Strategies. However, the high cost and lack of human clinical trials, makes gene therapy an apprehensive approach.
All the treatment options that are available so far provide only symptomatic treatment but fail to act at a cellular level. They fail to regenerate the wasted muscles or reverse the pathology of the disease.
Also, Muscular Dystrophy is a genetic disorder and hence no treatment can repair the core changes in the defective genetic structure.
Global research to treat muscular dystrophy has shed light upon the potential ability of cell to regenerate and repair the damaged muscle cells. cell are cells that are at an early stage of development. This means they have the ability to turn into any type of cell in the body and undergo self renewal.
Under physiological conditions the ability of adult muscle to undergo regeneration is largely attributed to a distinct subpopulation of muscle cells, termed satellite cells. These cells are considered to be the main cell type involved in skeletal muscle regeneration. Regenerative Medicine holds great promise as a treatment for Muscular Dystrophy by providing cells that can both deliver functional muscle proteins and replenish the stem pool.
Cell help counteract all the potential mechanisms that cause muscular dystrophy.
Transplanted cells have myogenic potential i.e. the cells can differentiate into a mature myocyte and therefore can repair and regenerate muscle fibers.
Preclinical evidence suggests that cell transplantation can restore dystrophin expression in mouse model of muscular dystrophy. Such dystrophin expression can lead to formation of muscle fibers that are resistant to easy damage and degeneration.
Exogenous cell transplantation replenishes the cell pool. Transplanted cells can also stimulate the resident satellite cells.
In addition to the actual regeneration of muscle cells and replacement of resident cell, transplanted cells also exhibit numerous beneficial paracrine mechanisms. cell secrete various anti-inflammatory cytokines and various growth factors that are myoprotective.
Vascular Endothelial growth factor is a growth factor that promotes angiogenesis.
In addition anti-inflammatory and neo-angiogenic effect, cells have immunomodulatory and anti-apoptotic effects on neighboring cells.
Transplanted cells also stimulate muscle plasticity and remodeling therefore prevents fibrosis . These paracrine effects are also catalyzed by exosomes secreted by MSCs.
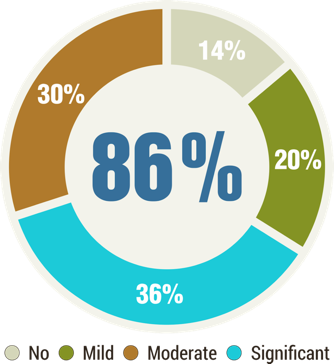
At, NeuroGen BSI, we have treated over 1500 patients of Muscular dystrophy with 86% patients showing overall improvements in the clinical symptoms. Muscular dystrophy is an emotionally, physically and financially draining condition, crippling not only the patient but others around as well. After years of research, regenerative medicine has emerged as an effective treatment option for this otherwise hopeless condition.
At Neurogen, for Muscular Dystrophy, the cell are injected into the various motor points of the patient, along with the intrathecal injection. Motor points are the point at which the motor branch of the innervating nerve enters the muscle. It is the point with the highest concentration of motor endplates and myo-neuronal synapses. It is the region of the highest number of neuromuscular junctions.
These points are identified and marked in each Muscular Dystrophy patient at the time of functional assessment. The cell are then injected at these points as well.
After transplantation our patients have shown have increased trunk muscle strength, limb strength on manual muscle testing and balance. Besides, they have also improvement in ambulation, hand function, increase in stamina and better trunk balance. Together, they make it easier for the patients to live more independently.
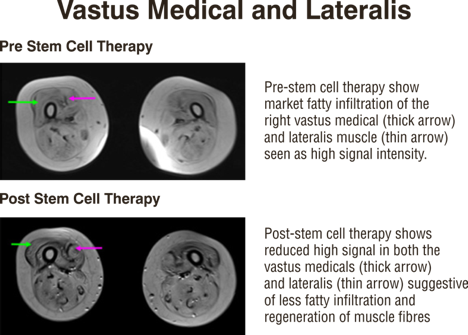
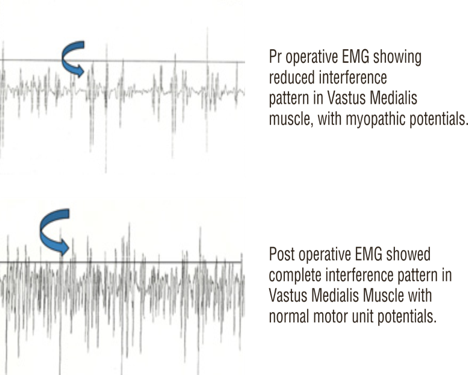
Our cell transplantation protocol does not only alter the clinical conditions of a patient, but also aims to repair and stop further progression of muscle wasting that occurs in Muscular dystrophy. This has been demonstrated by the MRI-MSK reports of these patients.
Objective radiological improvements seen in a case of muscular dystrophy after regenerative medicine
No, it is not a contagious disease. It is mainly a genetic disorder.
Not always. Many investigations state that about 1/3rd of all boys suffering from Duchenne/Becker's muscular dystrophy have no family history.
The most common type of muscular dystrophy is Duchene and second most common is Becker's. This is followed by limb-girdle muscular dystrophy which is the third most common form.
Most parents notice that the child is not running as fast as the other kids. The child may also get up from the ground, in a different way, using his hand for support and may have difficulty in climbing stairs.
Since muscular dystrophy is not a contagious disorder, it cannot be transmitted. However, it can be passed down from either of the parent via an affected gene.
In Duchenne Muscular Dystrophy the mother is a carrier of affected gene and the disease is usually transmitted to the male child. Each male born to such mother is on 50% risk of being affected and each female child born is at 50% risk of being a carrier.
In myotonic dystrophy, one of the parents is the carrier.
In limb-girdle muscular dystrophy, the transfer could be via a recessive gene, meaning both the parents are carriers, which means that both can transfer the gene. It could also be inherited as a autosomal dominant disease, that means that one defective gene is enough to manifest the problem/condition. Both male child and female child can be affected with the disease.
Yes. There are 50% chances of her being the carrier. Genetic testing for ascertaining it is available.
In utero diagnosis of Duchenne muscular dystrophy is possible, if there is history of previous child or sibling having this disease/condition is known. Chorionic villus sampling or amniocentesis followed by DNA testing (MLPA) can possibly give some answers.
If there is a family history and a reasonable suspicion, then maybe. However, the symptoms may not be apparent until the child is at least several years of age.
Not necessary. For example facioscapulohumeral, myotonic and limb-girdle muscular dystrophy begin later in life. They are slow in progression and less severe than the childhood forms.
In a few instances, such as facioscapulohumeral dystrophy a weak smile or inability to whistle may indicate a beginning. Similarly, in Limb-girdle muscular dystrophy weakness of shoulders and hip is seen and in case of Myotonic dystrophy there is apparent weakness of feet and hand.
The muscles are replaced with fatty or fibrous tissue. This condition is known as pseudohypertrophy.
A surgical release of tight or contracted muscle and immediately standing next day can help. Second option would be serial casting. These options can help children of muscular dystrophy to prolong walking independently.
Regular physiotherapy/exercises can help keep the child ambulatory. Standing with the help of push knee splints and high boots is found to be effective. Surgery becomes the best option when the muscles become very tight and are not stretchable at all.
A surgery can help straighten the joints. Surgery becomes the best option when the muscles become very tight and are not stretchable at all. However, walking would depend on the muscle power of the lower limbs.
These therapies help in preventing contractures, keep muscles strong, help in transfer, improve efficiency of functional activities like standing, walking etc.
If exercises are done beyond the patients' capacity, they can lead to deterioration. The patient should not get tired or fatigued. Ample time or rest has to be given between exercises.
Swimming is found to be a very good exercise for the child/patient of muscular dystrophy. It is advised to be brought into practice from a very early age. Helps to increase endurance, increases muscle strength and good work up for the respiratory and cardiac muscles.
Respiratory muscle weakness, leading to respiratory difficulty is the major cause of death. As the muscles weaken, the child develops scoliosis or bending of the spine. This leads to crowding of the muscles of the chest and the ribs. Cough reflex becomes hampered. Patient becomes prone to chest infection, which leads to breathing difficulty.
Cardiac muscle weakness and cardiomyopathy, leading to heart failure and is another major cause of death in muscular dystrophy patients.
The aim of Regenerative Medicine is to strengthen the muscles, prevent or slow down the degeneration of the muscles . If the patients is ambulatory/walking, the goal is to keep them walking. This indirectly could delay respiratory muscle weakness and prevent scoliosis. This could then prolong overall life expectancy , by reducing the chances of respiratory complications.
The biological task of cell is to repair and regenerate damaged cells. Regenerative Medicine exploits this function by administering these cells in high concentrations directly in and around the damaged tissue, where they advance its self healing and repair.
Bone marrow transplantation has been used successfully for genetic disorders of blood, such as sickle cell anemia, thalassemia, as well as cancers such as leukemia. Since our therapy uses these very cells, which are harvested from the patient's own body (autologous cells), there are no major ethical concerns. Ethical concerns are primarily on the use of embryonic cell (which we do not use).
The procedure is done under local anesthesia and a mild sedation. There is no significant pain or discomfort during or after the procedure.
Regenerative Medicine is minimally invasive and reasonably safe. None of our patients have shown any neurological deterioration so far in connection with the regenerative medicine itself. Some short-term side effects, such as headache (spinal headache) lasting 3-4 days which is generally self limiting, neck/back pain, vomiting, some mild rash or pain at the site of bone marrow aspiration/cell injection may occur. However, like any other medical or surgical treatment unexpected complications are always a possibility. These complications may be related to the medicines given, the cell procedure, the anesthesia, and the rehabilitation or to any of the pre-existing medical or neurological conditions.
Maximal improvements are seen around 3-6 months after the treatment. However, in many patients there are slow progressive improvements that continue for several months/years later. Most patients do show some immediate improvements also i.e. before the discharge, in some of their symptoms.
The decision to do the therapy a second time is taken after seeing the progress/improvements after the first therapy. If the patients show some encouraging improvement, then the case is reviewed by the entire medical and rehabilitation team and a second treatment may be recommended. This may be done anytime between 3-6 months of the first therapy.
We will review what other medications the patient is already on. In most cases we do not discontinue any already going on treatment. Please inform us about any medications you are taking beforehand.
This is difficult to predict, since this a relatively new therapy. It depends on multiple factors such as age of patient, type of illness, duration of illness and extent of rehabilitation taken after the treatment.
At Neurogen BSI, we have treated over 1400 patients of Muscular dystrophy. Over all improvements were seen in 94% patients.
We have published our results in "Cell Transplantation" - an international journal. This paper reports our clinical results in 150 patients of muscular dystrophy (DMD, LGMD, BMD) who were administered autologous BMMNC intrathecally, followed by multidisciplinary rehabilitation. Evaluation after transplantation showed improvements in the trunk muscle strength, limb strength on manual muscle testing, gait improvements, positive changes in the assessment scales such as the FIM and the Brooke and Vignos Scales
Our data is regularly published in various medical and scientific journal (available for reading on our website). You are strongly advised to study these before proceeding with treatment.
Case Report 1
Master MR who is a 5yr old child residing in Kolkata, is a known case of Duchenne Muscular Dystrophy (DMD). Since birth there were a few movements which he could not perform, which went unnoticed by his parents. An abnormality first became evident to them when he was 3 years old. It all began with difficulty in climbing stairs and not being able to pull himself upright from a sitting or sleeping position, running slowly, etc. He was seen by several experts in Kolkata but a clear diagnosis was never achieved. When he was around 4 yrs old, he was taken to a neurologist in Vellore where he was finally diagnosed with Duchenne Muscular Dystrophy based on clinical investigations. On understanding the grave implications of DMD the family was understandably devastated and found difficulty coping with the reality of the situation. "Watching your growing child deteriorate, suddenly facing difficulty in simple tasks like climbing stairs, pulling himself upright and gradually becoming dependent on you for Activities of Daily Living (ADLs) is heart wrenching" says his father. His mother was shattered emotionally. Their well wishers supported them, saying that God will show them the path to recovery soon.
Thus, began their quest for a treatment overall in India, including at Vellore, where they requested the doctors to help treat their child. The family finally came to hear about NeuroGen Brain & Spine Institute, through an article in a leading newspaper. They immediately got in touch with Dr.Nandini Gokulchandran and Dr.Alok Sharma through email and after discussing their son's case in detail they decided to visit NeuroGen in December 2015.
On further examination at NeuroGen BSI, Mast. MR was found to have the following problems:
Partially dependent in all ADLs (Activities of Daily Living)
Difficulty in climbing stairs
Difficulty in running and walking
Difficulty in comfortably pulling himself upright from seating or sleeping position. (Positive Gower's sign)
Abnormal thickness and tightening in calf muscles
Abnormal gait (waddling gait)
Lower limb (strongest muscles of the body), the hip muscles and inner thigh muscles were affected
Poor breathing capacity
Moderate Walking balance
Poor stability and mobility of trunk muscles like abdominals and back extensors
Difficulty in performing hand functions
Difficulty in bed mobility
Poor standing balance
Affected speech (stammering)
Difficulty in cycling or balancing on one leg
Poor stamina, easy fatigue
Frequent falling
Occasional bed wetting
MR underwent Cell Transplantation on 15th December 2015. "We were told that the regenerative medicine would take around 3-6 months to show its results. We were guided in detail in terms of the therapies which needed to be continued and a certain diet chart needed to be followed along with medications. Being at NeuroGen and meeting Dr.Alok Sharma and Dr.Nandini Gokulchandran gave us a lot of hope and motivation to fight my child's disorder" said MR's father.
MR has been doing 4-5 hours of therapy in a day. Within two months after discharge he had started showing tremendous improvements and had reached approximately a 70% improved stage. On a telephonic follow-up with his parents, it was found that he had shown the following improvements.
He had started cycling with his friends which he was unable to do earlier.
Standing and walking balance had improved including being able to stand on one leg.
He could run properly and play with his friends.
Qualitative improvements were noted in terms of shifting himself on his own. He needed to put in lesser efforts for bed mobility activities like rolling and getting up from sleeping position.
His stammering reduced, and hence speech become almost normal.
Upper limb activity like dressing himself, brushing his teeth etc. became easier.
Gait and posture improved.
His calf muscle hypertrophy reduced.
Stamina improved - earlier he used to so only 1-2hrous or therapy but after the treatment he was able to do 4-5 hours of therapy sessions every day.
His frequent falls had almost stopped.
Bed wetting had completely stopped.
"We are ecstatic that our son's condition has improved, for whom other doctors had given up hope. Our experience with NeuroGen was good. Dr.Alok Sharma and Dr.Nandini Gokulchandran are very helpful and supportive. We have already recommended many parents with special children to consult NeuroGen for their child and try for regenerative medicine" - concluded his father.
Case Report 2
Master SB is a 20 yrs old male and a known case of Muscular dystrophy. His symptoms started at 12 yrs of age, with difficulty in walking, sitting and getting up from a sitting position. When he was 4 yrs old, his father noticed initial symptoms of muscle weakness in him. Since he had a strong family history of muscular dystrophy from his maternal side, his father did not take any immediate action, as they had seen a discouraging progression of the disease in their relatives' cases. At the age of 8, however, his father got a complete check up done for him from a neurologist and hence he was formally diagnosed with Muscular Dystrophy. SB was given medications by the doctor in Indore. On realizing that his condition was gradually worsening, they visited several doctors but everyone prescribed medications only. "We by ourselves decided to start some basic physiotherapy for him but that did not last long, eventually when he was 12-13 years old we stopped all his medications". They also tried Ayurveda for 2-3 years but that worked negatively for him; his condition started deteriorating and they stopped with all the therapies, medications and ayurvedic treatment.
In the year 2015 while browsing for muscular dystrophy treatments, SB and his father came across Regenerative Medicine at NeuroGen Brain and Spine Institute in Mumbai. They contacted NeuroGen and did a thorough discussion on phone and email with Dr.Alok Sharma and Dr.Nandini Gokulchandran.
On understanding all the details Shubham underwent Regenerative Medicine at NeuroGen BSI in December 2015. On examination below problems were noticed:
His early symptoms included falls, toe walking.
Difficulty in getting up from floor and chair.
Difficulty in climbing stairs and walking since 2-3 years.
Tightness in calf muscles
Improper gait
Poor aerobic capacity
Poor standing and walking balance
Weakness of muscles in lower limb
Difficulty in pulling himself upright from seating or sleeping position. (Positive Gower's sign)
Stamina was poor.
At NeuroGen, SB underwent Regenerative Medicine along with a customized rehabilitation program. The aim of the rehabilitation program was to develop dissociations and gait training, therapies to increase the strength of the affected areas without fatigue and to increase overall stamina of the patient. He was given exercises that would help him improve his balance, walking, stair climbing, rolling, posture and his grip. These exercises carried out in a systematic pattern with sufficient rest intervals to the patient. Together, the aim of the rehabilitation program was to improve his overall quality of life. SB and his family found new hope with NeuroGen's Regenerative Medicine. They were motivated and positive for him after going back. Physiotherapy and rehabilitation taught at NeuroGen were continued after going home.
Improvements seen in SB after 4 months of Regenerative Medicine are as follows :
Reduced waddling.
Improved speed.
Reduced toe walking.
Improved standing balance.
Improved walking balance.
Better possibility of getting up from a sleeping condition.
Supine position to sitting improved.
Bed mobility activities improved and became easier.
Started climbing using railing, but efforts reduced.
Could perform sit to stand more easily.
All fours limb movements improved.
Needed less effort in coming to kneel position.
Improved stamina.
Improvement was seen in qualitative ADL.
Falls had reduced, earlier 1-2/day, now has 1/15 days now.
Meter walking time improved from 316 meters to 330 meters.
After all that SB had gone through, these improvements allowed him to emotionally improve as well. His confidence increased and he was able to do all his daily tasks with enthusiasm and motivation. Fear of falling went away. "We are very happy and satisfied with Regenerative Medicine at NeuroGen. It has given us a hope that there is a treatment which can make my son's life easier to live. At NeuroGen all the doctors and the staff are so cooperative and helpful. The guidance we wanted since long has been received at NeuroGen. How to take care of him and maintain his condition was explained to us. He is doing regular physiotherapy now and is also pursuing his studies", concluded his father.
