- +91 99202 00400 / +91 22 4113 6565
- contact@neurogen.in
Disclaimer: At NeuroGen BSI, autologous bone marrow tissue, after minimal manipulation, is grafted by medical practioners as part of routine procedure within the hospital in the same surgical sitting. According to the directives of the Ministry of Health and Family Welfare issued under section 33P of the Drugs and Cosmetics Act,1940 this procedure does not involve use of stem cells/ stem cell derived product.
Autism is a developmental disorder which is characterized by impairments in speech, verbal and non‐verbal communication, and emotional development. It may also include meaningless sounds and repetitive behavior.

Autism Spectrum Disorder (ASD), on the other hand, is an umbrella term coined for a group of neurodevelopmental disorders that essentially affect behavior, communication and social interaction of an individual. The most commonly occuring ASD is Autism.
Autism Spectrum Disorder can be different combinations of different symptoms, and the severity of symptoms and functional independence, can vary. Depending on these factors, the other disorders that can be categorised under ASD are, Asperger's Syndrome, Rett Syndrome, Pervasive Developmental Disorders‐ Not Otherwise Specified (PDD‐NOS), etc.
Generally, parents notice signs of ASD very early before age 2 or 3. Usually, it is noticed that the child's motor milestones are time‐appropriate, however, they either lag, or show a regression of their cognitive milestones, such as speech, eye contact, interaction, etc.
Autism Spectrum Disorders can be caused by several genetic and/or environmental causes. Several studies are being conducted globally, to ascertain the exact genetic markers or causes of ASD, but unfortunately, no definitive answers or explanations have been found.

It has, however, been observed that environmental causes, such as, rapid increase in air pollution can lead to heavy metal accumulation which could contribute to ASD. Another commonly observed theory suggests lack of oxygen immediately after birth.
There have been studies to connect gut related issues to Autism as well, and while a modified diet does show improvements in its symptoms, no definitive cause as such has yet been derived.
The earliest sign of ASD is a lack of responsiveness. The child neither responds to its name, nor does it attempt to make eye contact. There is a lack of imitation of actions, speech or facial expressions. Additionally, speech delay and lack of interaction are also observed.
Some children show regression in symptoms; they show normal development till a certain age and then regress in terms of speech, eye contact and learning. Many parents feel like the child is "lost in its own world". They seem unconnected to others even around their families.
Certain medical and mental health issues (comorbids) frequently accompany ASD. They include gastrointestinal (GI) disorders, seizures, sleep disturbances, attention deficit and hyperactivity disorder (ADHD), anxiety and phobias.

The Autism and Developmental Disabilities Monitoring (ADDM) Network of the Centers for Disease Control and Prevention (CDC) has updated the prevalence of Autism Spectrum Disorders from 1 in 68 children in 2012, to a staggering 1 in 59 children in 2014, which clearly indicates that the incidence and prevalence of autism is on the rise. It is above 4 times more common in boys than in girls.


ASD can be detected on the basis of clinical symptoms and is usually diagnosed by family physicians or pediatricians. The school teacher or primary caregiver might recognize these signs and consult their family doctor.

There are no definitive curative treatments available for ASD. Management of the disorder is mainly through symptomatic medication. Traditional medical treatment options include medicines to manage symptoms such as hyperactivity and lack of attention.

Rehabilitation therapies form the mainstay of treating Autism. Applied Behavior Analysis, Occupational Therapy, Speech Therapy, Special Education, etc. are useful in enhancing the functioning of individuals with ASD and improving their quality of life.

However, none of these treatments address the core pathology of ASD, and thus, none of them provide a cure for the disease. Therefore, there is a burning need for treatment strategies that can have an effect on the core disease pathology and help reduce the symptoms of ASD.
In the recent years, regenerative medicine is one such treatment method, which as has shown a glimmer of the possibility of altering the core pathology as well as providing symptomatic improvement in children and adults with Autism.
Recent studies have indicated that the lack of oxygen supply to the brain during or after birth, and immune deregulation, are the two important factors associated with ASD. These factors may result in irregularities or a decrease in brain function. This can cause an overarching imbalance in the brain which could manifest as the various symptoms of ASD.
As brain functioning is heavily involved in ASD, scientists and researchers have started looking at regenerative therapy using cell as potential therapy for ASD. cell have the capability to multiply into many cells and form specialized cells different from the mother cell. This regeneration of cells can help in repairing the damaged brain tissue.

Cell have the potential to repair the affected neural tissue at the molecular, structural and functional level. They are known to address the core of neuropathology of ASD with the help of their unique paracrine regulatory functions that are capable of regulating cell differentiation, tissue and organ repair, neurotrophic and anti‐inflammatory actions in the recipient.
Regenerative Medicine using autologous bone marrow derived MNC's has shown significant clinical and objective radiological improvements in children with ASD. It is simple, safe and effective treatment modality as it focuses on neurological repair. It gives a new life to these children and helps integrating them back into society.
The regenerative medicine done at NeuroGen has resulted in several remarkable improvements in various symptoms of ASD. Hyperactivity and engaging in stereotypical and repetitive motor mannerisms decrease significantly. Sensory and motor functioning improves. Improvements are seen in concentration and the attention span.
The overall improvements that are seen in patients after regenerative medicine are:
Reduction in self stimulatory behavior
Improvement in eye contact
Improvement in speech
Improvement in speech and communication skills
Improvement in social interactions
Reduction in aggressive and self‐injurious behavior

Changes in clinical symptoms can be correlated with the improvements in the brain metabolism as well that is observed in the PET‐CT (Positron emission tomography‐ computerized tomography) scans.1
PET CT Scan improvements


Pre cell treatments PET CT scan show the blue areas that represent reduced brain activity due to the damage that occurs to the neural tissue in ASD.

Post Cell Treatment PET CT scan show the blue areas have reduced indicating that the damaged tissues have been repaired highlighting the positive effects of the regenerative medicine.
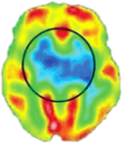
PET CT Scan of the Brain before Regenerative Medicine shows Blue areas that Represent reduced brain activity due to the damage that occurs to the brain tissue in Autism.

PET CT Scan of the Brain 6 months after Regenerative Medicine shows that the blue areas have reduced Indicating that the damaged tissues have been repaired Highlighting the positive effects of Regenerative Medicine.
Parents of children with ASD usually have common questions when they consult their pediatrician or child psychiatrist. How did our child develop ASD? My child was hale and hearty and had even started to speak a few words. What happened suddenly? So, is ASD acquired? Does it happen after the child is born? Could it have been prevented? Is it genetic? Can the other children also have ASD? Has it come from "us", the parents?
The truth is that several research studies to explore all possible causes of Autism are ongoing. Some combination of genetic, biological and environmental factors is believed to cause ASD. Researchers are now, however, exploring several genes which are believed to contribute to the development of these disorders as well as several regions in the brain that have been linked to the disorders.
Your child might have ASD because of some combination of these reasons. There might be a genetic reason or some biological or environmental factor that might have lead to your child having ASD.
Genetic factors are believed to be a major component contributing to the cause of Autism Spectrum Disorders. Heritability was established, very early on, in a study on the occurrence of ASD in twins. Explaining the occurrence of ASD, purely on the basis of genetics is a very complex task. Though various molecular tools and analytical tools (such as linkage analyses, association analyses) have tried to be used, nothing very conclusive has emerged. Since, more than one gene has been implicated or found to be involved, a simple arithmetic or cause and effect, cannot be established. Researchers are also exploring the effects of genetic imprinting in which a gene's expression is determined by which parent donates the gene copy. However, there are no definitive answers to this question.
Researchers from Aarhus University in Denmark have reported in a journal JAMA Pediatrics that children with an older brother or sister diagnosed with an Autism spectrum disorder are more likely to be on the spectrum themselves. Siblings who shared the same mother and father had a 7.5 greater risk of having ASD, whereas maternal half siblings had a 2.4 greater risk. Paternal half siblings didn't have a statistically significant increase in risk. Hence, it's important that parents who already have a child diagnosed on the spectrum should consider this while planning for another child. They should inform the doctor about their family history before conceiving another child and should take precautionary measures such as taking prenatal folic acid and avoiding overexposure to toxins.
There is no known 'cure' for ASD. This does not mean, however, that it cannot be treated. There are medications and therapies that can help people with ASD function better. For example, medication might help manage very high energy levels, inability to focus, depression, or seizures and behavior therapy can help parents manage the difficult behaviors in their child. When these therapies are accompanied with regenerative medicine, they are known to show better outcomes.
No, medicines cannot cure ASD. However, medicines can help manage various symptoms of ASD. You should consult a pediatrician or a psychiatrist if your child has difficulty controlling aggression, displays self‐injurious behaviors, frequently throws temper tantrums, has repetitive behaviors or quickly changing moods.
Treatment of symptoms is very important as they restrict independence and quality of life of people with ASD, their families and caregivers. Once the symptoms are controlled with medications, there is a better scope for benefit from multidisciplinary interventions like Applied Behavior Analysis, Occupational therapy, psychological therapy, speech therapy, vocational training, etc.
A common dilemma that bothers several parents of children with ASD is that of their child's formal education. Due to lack of clear cut guidelines, parents are unable to decide what type of schooling system is best for their child.
Off late, the number of schools providing education to children with ASD has bettered over the years. Broadly speaking schools may be categorized into the following:
Mainstream or Regular,
Inclusive or Integrated,
Special services schools,
Home‐schooling,
Residential schools or homes.
Children with ASD generally have a very tough time with large groups, loud, stimulating settings, and poorly managed transitions. As the child grows older, a typical classroom can be very challenging. A one to one type of schooling is best suited for children with ASD. As they grow older and their skills improve, they can be transitioned into a normal classroom or inclusive classroom.
As parents, you may frantically look for all possible treatment options for your child. Your search may lead you to several options which may further confuse you or create more doubts. With help from your developmental pediatrician, you may be able to identify the problems in your child and curate an early intervention plan.
Early identification has become more important than ever, as many studies have found that children with ASD, who receive services prior to 48 months of age, make greater progress than those who enter treatment programs after 48 months of age.
Management of ASD calls for a multi‐disciplinary and holistic approach. This consists of:
Clinical Psychologists
Occupational therapists
Speech and language pathologists
Dieticians
Physiotherapists
Art, play, music, drama therapists
Each of the above professionals will target different aspects in the treatment of your child.
There are newer forms of therapies also which have been proven to be very effective like Regenerative Medicine, Hyperbaric oxygen therapy (HBOT), etc.
Bone marrow transplantation has been used successfully for genetic disorders of blood, such as sickle cell anemia, thalassemia, as well as cancers such as leukemia. Since our therapy uses these very cells, which are harvested from the patient's own body (autologous cells), there are no major ethical concerns. Ethical concerns are primarily on the use of embryonic cell (which we do not use).
Regenerative Medicine is minimally invasive and reasonably safe. None of our patients have shown any neurological deterioration so far in connection with the regenerative medicine itself. Some short‐term side effects, such as headache (spinal headache) lasting 3‐4 days which is generally self limiting, neck/back pain, vomiting, some mild rash or pain at the site of bone marrow aspiration/cell injection may occur.
However, like any other medical or surgical treatment unexpected complications are always a possibility. These complications may be related to the medicines given, the cell procedure, the anesthesia, and the rehabilitation or to any of the preexisting medical or neurological conditions.
Maximal improvements are seen around 3‐6 months after the treatment. However, in many patients there are slow progressive improvements that continue for several months/years later. Most patients do show some immediate improvements also i.e. before the discharge, in some of their symptoms.
The decision to do the therapy a second time is taken after seeing the progress/ improvements after the first therapy. If the patients show some encouraging improvement, then the case is reviewed by the entire medical and rehabilitation team. Certain special imaging tests, such as PET CT Scan of the brain, would be repeated and then a second treatment may be recommended. This may be done anytime between 3‐6 months of the first therapy.
We will review what other medications the patient is already on. In most cases we do not discontinue any already going on treatment. However this is decided on a case by case basis. Please inform us about any medications you are taking beforehand.
At NeuroGen BSI we have successfully treated over around 1200 cases of ASD. We have published the world's first clinical study of 32 patients in the International Journal "Cell International". The results published in this path‐breaking paper demonstrated that cell are safe and efficacious in ASD.
Within the first three‐six months, our patients have shown improvements in social relationships, emotional responsiveness, speech and language, communication, behavior patterns, reduced hyperactivity, repetitive motor mannerisms, sensory problems and attention and concentration.
Our data is regularly published in various medical and scientific journal(available for reading on our website) . You are strongly advised to study these before proceeding with treatment.
The biological task of cell is to repair and regenerate damaged cells. Regenerative Medicine utilises this function by administering these cells in high concentrations directly in and around the damaged tissue, where they advance its self healing and repair.
The therapy is done under local anesthesia and a mild sedation. There is no significant pain or discomfort during or after the procedure.
Case report 1
Master LV, an 11 yr old child from London, was diagnosed W ASD, when he was 4 and a half years old. In the UK he received the best treatment as well as rehabilitation therapies available. However, for almost 5 years, his parents did not notice any significant improvements in him.
He had the following symptoms:
Poor social interaction
Fleeting eye contact
Inappropriate emotional responses, such as irrelevant laughing and crying without any reason
Motor mannerisms, such as finger fidgeting, rocking
Smelling objects
Presence of unusual noises
Fearful of loud noises
Weak fine motor skills
Poor to fair perceptual and cognitive skills
After undergoing regenerative medicine he has shown remarkable improvements in perceptual and cognitive skills. He now has better eye contact, an increased attention span and an increase in general awareness. There have been improvement in sensory problems and his motor mannerisms have reduced in public places. His social interaction and communications are better now. He has become more independent with his activities of daily living. His learning and comprehension have improved tremendously, such that now he is able to solve a 100 piece puzzle in less than 5 minutes. A child who had low tone and severe imbalance issues, can now skate like a professional!
All this has been possible only after regenerative medicine. LV'S life has changed for the better.
Case report 2
Mast AM was 6 year old when he came to NeuroGen in October 2016 to undergo regenerative medicine, for his ASD. He had significant impairments in eye contact, cognition, socializing, speech, self‐ help skills, and sitting tolerance. His mother reported that his emotional responses were excessive in terms of irrelevant laughing. He engaged in smelling and mouthing objects. He had tactile, vestibular, proprioceptive, auditory, and olfactory hyposensitivity to sensory inputs. He would tap or bang objects, run around the room, and climb on furniture. He had vocal stimming and would keep saying meaningless things or humming all the time. His speech was not age‐appropriate and was unclear. His parents and other caregivers would understand him but it was difficult for a new person to understand what he was saying. He would communicate mostly in 1 or 2 words phrases.
Another major issue was that he would stay aloof and not interact with his classmates. He could not interact correctly with them. He was dependent for his self help skills and was not toilet trained. His assessment test scores also indicated moderate severity of ASD. On the Indian Scale for Assessment of ASD (ISAA), his score was 115 while his Childhood ASD Rating Scale (CARS) score was 33 which indicates moderate level of ASD.
They came back to NeuroGen after 6 months for a second shot of Regenerative Medicine. He showed significant improvements in this duration. He could now follow 2 or 3 step commands, he would stay with his mother and not elope in public places, which used to a be a great safety concern for his family while going out, earlier, and his attention and focus had improved. He had started showing some interest in other children and would now follow his peers around. His play skills also improved. And he learned to wait in line for his turn.
His emotional understanding improved. He started reading facial expressions and reacting appropriately to others which gave his parents the sense that he could now "connect" better with them. His hyperactivity reduced and he could sit longer for non‐preferred activities. His irrelevant laughter decreased. His running around the room, jumping, banging and throwing things, and vocal stereotypical behaviors reduced. His mouthing behavior completely stopped. Academically, his reading improved namely, he could read 2 letter words. He learnt to identify numbers upto 25. He developed interest in painting. He became more independent in bathing and dressing. His fine motor skills improved due to which he was able to button his shirt. In terms of eating, his would eat a variety of food. He started choosing and expressing his preference with what he wants to eat.
In terms of scores and objective data, ISAA score showed a marked reduction from 115 to 76. CARS score reduced from 33 to 30. These scores show that there were amazing improvements after Regenerative Medicine and he was more independent.
